

Abstract
INTRODUCTION: Although diffuse large B cell lymphoma (DLBCL) is considered a curable disease in the immunochemotherapy (ICT) era, about 40% of patients relapse or are refractory to first line treatment, representing an unmet clinical need. The role of upfront autotransplantation (ASCT) in high-risk cases is still debated, while its role in relapsed/refractory (R/R) disease is established in all guidelines. However less than 50% are actually cured with salvage ASCT (Gisselbrecht C et al, J Clin Oncol. 2010) and outcome of patients who relapse after ASCT is very poor (Crump M. et al, Blood 2017; Van Den Neste E et al, BMT 2017). Prognosis of aggressive lymphomas with characteristics intermediate with Burkitt's lymphoma (BCLU), recently reclassified (WHO 2016) as high grade lymphoma, unspecified with or without c-myc translocation, is less favourable. Regimens containing HD-MTX/ARA-C were generally used to treat these lymphoma subtypes as well as lymphoma with central nervous system (CNS) localization. Aim of this study was to evaluate the prevalence and outcome of R/R lymphoma after upfront or salvage ASCT or after HD-MTX/ARA-C regimens in the clinical care setting and to identify potential salvage approaches.
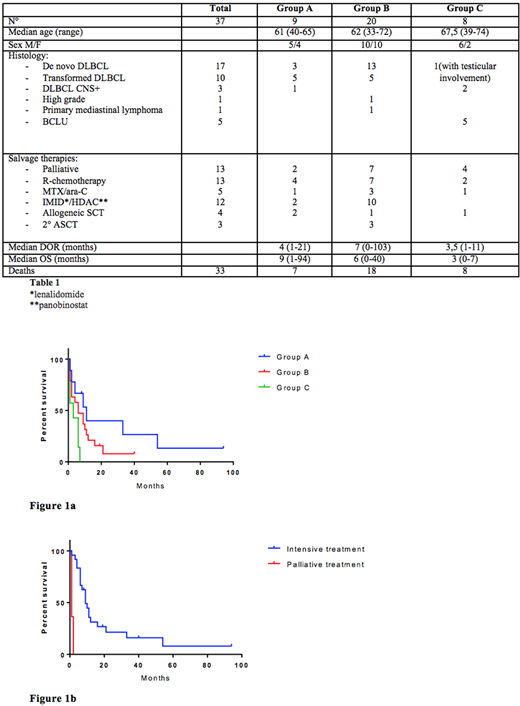
PATIENTS and METHODS: We retrospectively analysed all consecutive HIV-negative patients seen at our Institute from January 2008 to December 2016 with de novo or transformed DLBCL, Primary mediastinal B-cell lymphoma or high-grade lymphoma/BCLU. First-line treatment used was R-CHOP/CHOP-like regimens. Consolidation with ASCT was performed in all high/intermediate-high IPI risk patients less than 65 years old, while salvage ASCT was performed after salvage ICT for R/R disease; HD-MTX/ARA-C regimens were used in DLBCL patients with CNS involvement or in BCLU cases. Relapsed or refractory patients after upfront or salvage ASCT or after HD-MTX/ARA-C were selected and their demographic and histological features as well as their outcome was analysed in term of duration of Response (DOR) from ASCT or MTX/ARA-C regimen to relapse and Overall Survival (OS) from relapse to the last follow-up or death. We recorded salvage treatments carried out according to age, performance status, available clinical protocols or international guidelines (more than one line in some patients).
RESULTS: Among 571 patients consecutively seen during the time period, 156 (27.3%) proved refractory or relapsed after first-line treatment. ASCT was performed in 86 patients as consolidation (group A) and in 33 as salvage (group B). First line HD-MTX/ARA-C regimens were used in 16 patients (group C). Relapse occurred in 9/86 group A (10%), 20/33 group B (61%) and 8/16 group C (50%) patients respectively, representing 6.5% of the whole patients initially diagnosed. First relapse occurred after a median DOR of 4, 7, and 3.5 months in group A, B and C respectively. The main demographic and histological characteristics of relapsed patients are summarized in the Table 1, which also shows treatments used after relapse. Response rates in patients treated with curative intent were 29% (6/21). Mortality rates were high in all groups (78%, 90% and 100% respectively), with an OS significantly better in group A comparing to group B and C patients (p 0.0243) (Fig.1a) and in patients treated with curative intent compared to patients that received palliation (p <0.0001) (Fig.1b). Four patients only are currently alive, 2 in group A at 84 and 3 months after allotransplantation and 2 in group B at 15 months after HD-MTX/ARA-C for CNS recurrence and after R-DHAP ICT with lenalidomide maintenance still ongoing at month 36th as part of a study protocol. The cause of death for all patients was progression of disease.
CONCLUSIONS: This analysis shows the very poor prognosis of patients with aggressive lymphoma relapsing after high dose therapy (ASCT or MTX/ARA-C). The recurrence of disease in these patients is early and salvage therapies are ineffective in most of the cases, although trying to treat these patients with curative intent shows a survival advantage over palliation. Patients treated with multiple lines of chemotherapy (group B) or with upfront HD-MTX/ARA-C (group C) have the worse prognosis. These data justify intensive follow-up programs during the first year after the end of therapy, and underline the need to develop new therapeutic strategies for this setting of patients, which could represent an ideal indication for CAR-T cell treatments.
Rossi:GILEAD: Other: ADVISORY BOARD; SANOFI: Other: ADVISORY BOARD; NOVARTIS: Honoraria; ABBVIE: Other: ADVISORY BOARD; CELGENE: Other: ADVISORY BOARD; AMGEN: Other: ADVISORY BOARD; JAZZ: Other: ADVISORY BOARD; JANNSEN: Other; MUNDIPHARMA: Honoraria; BMS: Honoraria; PFIZER: Other: ADVISORY BOARD; TEVA: Other: ADVISORY BOARD; ROCHE: Other: Advisory Board; SANDOZ: Honoraria.

